So the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) sits on the calendar with a January 1, 2027 enforcement date, and your engineering lead just asked how you get from a whiteboard to a live Prior Auth API in half a year. The short version: it is doable, but only if you stop treating the four APIs as a single big-bang project and start treating them as four connected slices with their own risks. If you want more healthcare interoperability notes to hand around your team while you scope this, we keep a running set on the homepage.
What Actually Has to Go Live
Before anyone books a sprint, the team needs to be honest about scope. CMS-0057-F requires four API surfaces, each with its own Da Vinci implementation guide behind it:
- Patient Access API refresh, aligned with PDex
- Provider Access API for treating clinicians, aligned with PDex
- Payer-to-Payer API for member data portability
- Prior Authorization API using CRD, DTR, and PAS
Add to that the quarterly metrics reporting on PA volume, decision times, and denial rates. That reporting is what regulators will actually look at first, and it is the piece most payers under-scope.
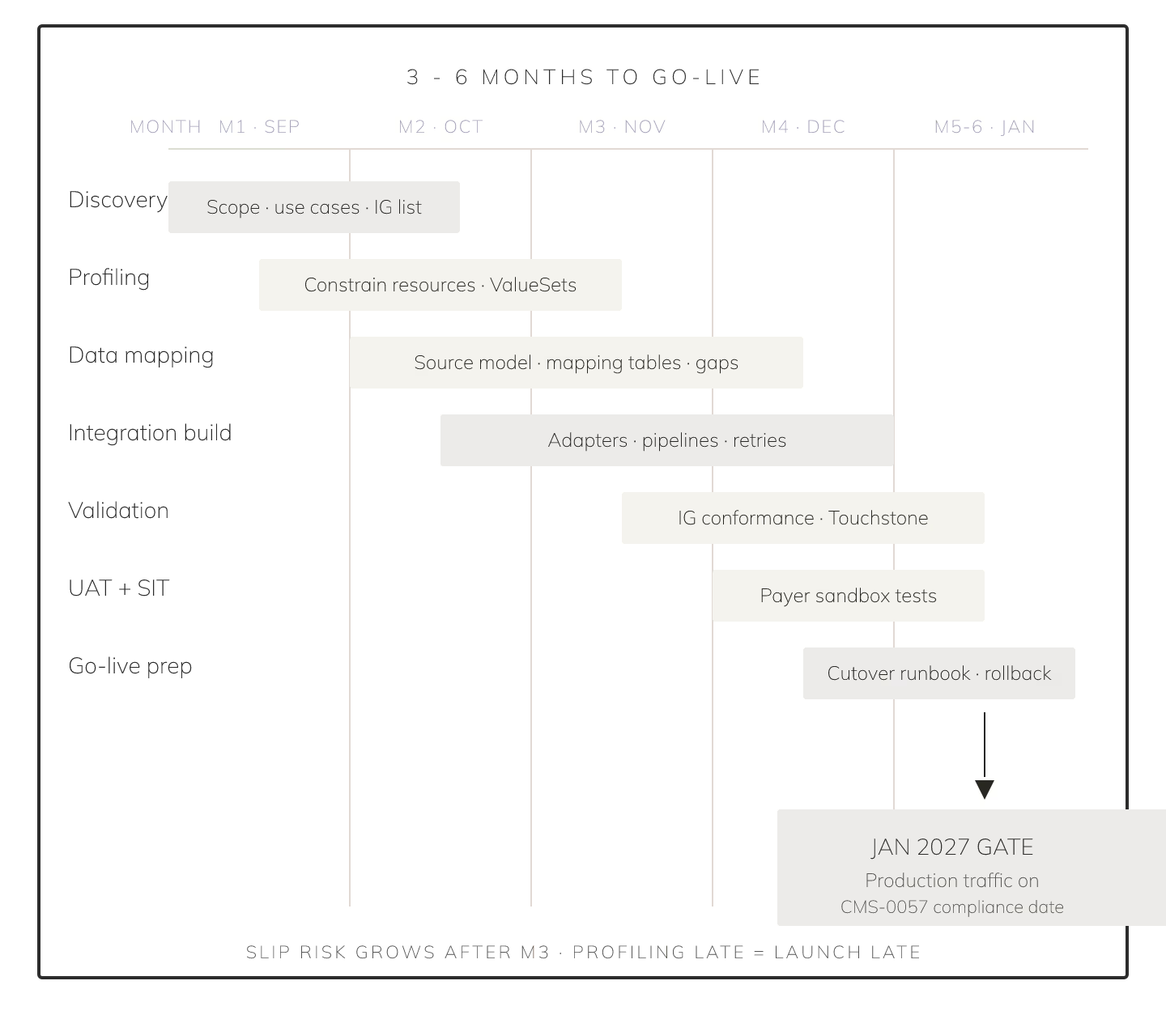
Month 0 to 1: Scope and Runtime Choice
The first four weeks are about discovery and one hard architectural call. You take an inventory of what already exists in-house: a claims system, a UM platform, whatever FHIR facade you may have from the 2020 CMS-9115 rule, and whether your terminology stack can carry the extra load. You also decide whether CMS-0057-F is a set of features layered on a FHIR runtime you already run, or a new separate compliance platform.
That choice sets the pace for everything downstream. In practice, in the embedded compliance camp, offerings like Payerbox from Health Samurai treat CMS-0057-F as a set of APIs to layer onto an existing FHIR core rather than a separate platform to procure. The other camp is per-API point vendors stitched together. Both can work; only one keeps you inside the six-month window if you also want the metrics reporting to be first-class.
Risks this month: unclear ownership between IT and compliance, and vendor demos that promise "certification-ready" without naming which IG version.
Month 1 to 3: PA API Core and Patient Access Refresh
Now you build the meat. Provider Access MVP comes online with a member attribution feed and a $everything endpoint. Patient Access gets refreshed to include claims, encounters, and clinical data per the updated PDex profile. The Prior Auth API core starts with CRD for coverage requirements, DTR for documentation templates through a SDC-style Questionnaire flow, and PAS for the request submission itself. If you are picking a form runtime for the DTR piece, our notes on medical form builders for multi-site GP practices in 2026 walk through the same trade-offs UM teams face.
Risks: over-optimizing the DTR forms before you have a single end-to-end PA submission working. The truth is you want ugly-but-working before pretty-and-broken.
Month 3 to 4: Payer-to-Payer and Metrics Scaffold
Payer-to-Payer looks scary and turns out to be the tamest of the four, since it reuses the Provider Access data model against a different consent surface. Book two sprints for it. In parallel, the metrics pipeline starts recording every PA transaction so that when Q1 2027 closes, the numbers already exist. Bolt-on ETL projects for the metrics are a common trap; the vendors that treat metrics as first-class outputs save you a quarter of engineering time. A companion piece on vendors for CMS bundled payments PROMs compliance in 2026 covers the same "compute-as-you-go" pattern applied to a different rule.
Risks: consent capture edges (opt-in vs opt-out) and the temptation to defer metrics until "the APIs are stable".
Month 4 to 6: Hardening, Certification, Soft Launch
The last stretch is unglamorous and non-negotiable: SMART on FHIR scopes, OAuth2 flows for member and provider apps, audit logging, load tests against a realistic PA volume, and a certification dry run through the Da Vinci reference validators. Soft launch means one payer partner and one provider group before you open the gates.
Risks: leaving security to the final month, and skipping the reference-validator run because "the demo passed".
Who This Timeline Fits
Six months is the floor, not the average. If your team owns a FHIR runtime and can dedicate four to six engineers plus a compliance lead, this playbook lands you at soft launch by month six with room to breathe before the January 1, 2027 deadline. If you are still choosing a FHIR runtime in month one, the honest answer is you are looking at nine months, and you should plan accordingly.
Sources
- PDF, CMS, 2024 - Fact Sheet on the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) with impacted-payer scope and 2026/2027 compliance dates
- PDF slides, CMS, 2024-03-26 - CMS-0057-F Final Rule presentation covering Patient/Provider/Payer-to-Payer/Prior Auth APIs and metrics reporting
- HTML IG, HL7 Da Vinci, STU2.1 - Prior Authorization Support (PAS) FHIR Implementation Guide, current published version referenced by CMS-0057-F